When people who’ve never experienced it think of chronic pain, they tend to only consider the most obvious symptom – pain. However, it usually comes with a whole host of other non-pain related issues, such as fatigue, brain fog, sensory issues and insomnia, as well as psychological symptoms such as depression or anxiety. What’s more, people with chronic pain have to deal with way more practical and administrative tasks than the average person: making and going to various appointments, taking medication, remembering to order medication, etc. They may face discrimination at the workplace, struggle to advocate for themselves in medical settings, and feel misunderstood and dismissed in social interactions when their loved ones just don’t seem to get it.
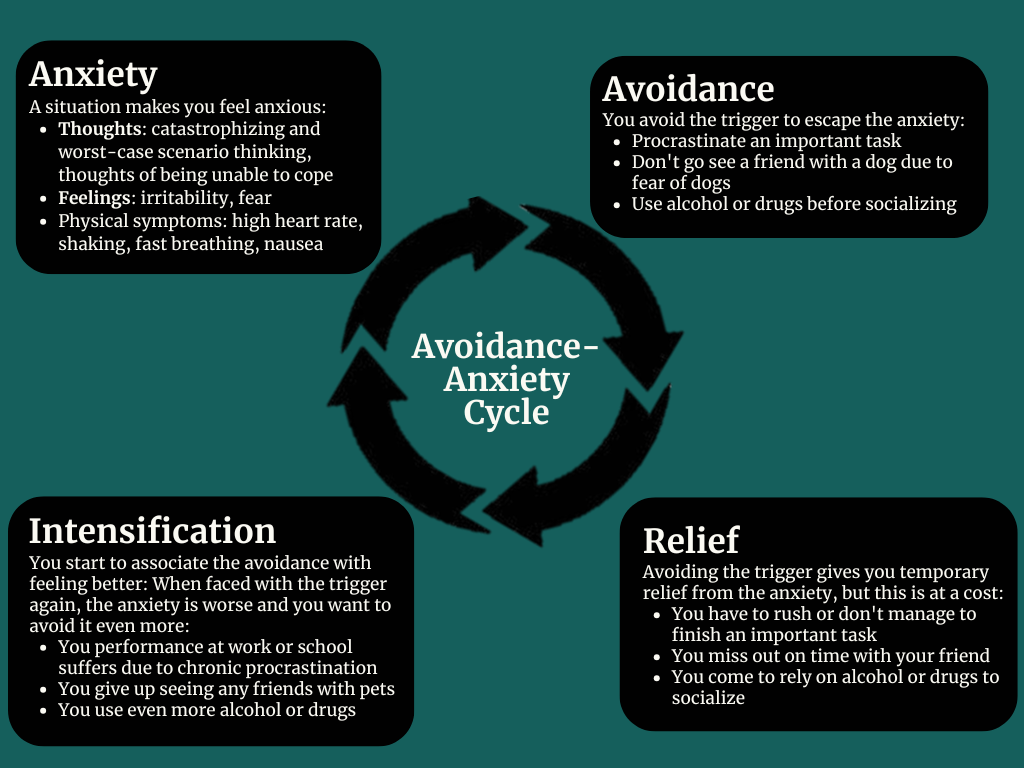
Therefore, it affects everything: the way you think, the way you feel, how you relate to others and how connected or disconnected you feel from the world around you. If you live with chronic pain, be it migraines, back pain, fibromyalgia, endometriosis or something else, you may notice the following cycle:
- The worse the pain gets the more you withdraw
- The more you withdraw, the more isolated you become, and everything feels harder
Indeed, research shows that mental health and social support play an important role in how we experience and cope with pain.
Chronic pain is more than physical
Chronic pain conditions are quite common, and often disabling. At the same time, they are frequently associated with psychological factors like stress, anxiety and depression.
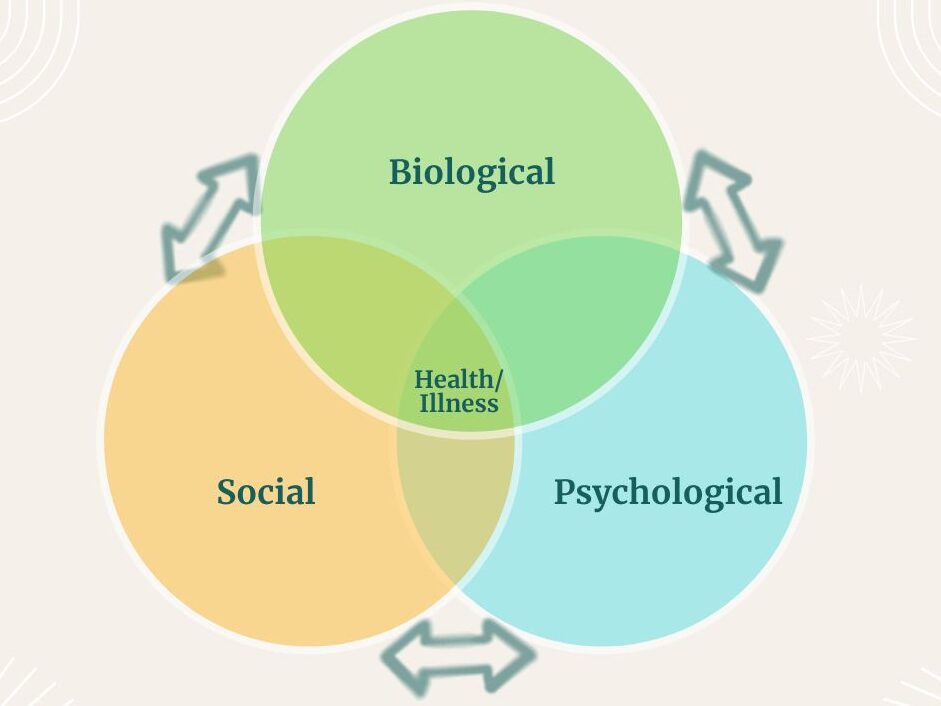
This is where the biopsychosocial model comes in, which in simple terms means that the pain, and the experience of pain, is shaped by biological, psychological and social factors.
Taking chronic migraine as an example:
- Biological factors might be: genetics, hormones (menstrual cycle), or an injury, such as a concussion
- Psychological factors might be: high levels of stress, anxiety disorder or avoidant coping style
- Social factors might be: loneliness, discrimination or work environment
The hidden link: pain and loneliness
One of the most important, yet often overlooked, factors influencing the experience of chronic pain is perceived social isolation. That means feeling alone, even if you are not necessarily actually alone. You can have friends and/or a partner and be part of a larger community, yet still feel misunderstood and lonely. Subjective loneliness is strongly linked to worse outcomes in both physical and mental health, so it really matters, if we try to look at chronic pain treatment from a holistic lens.
How isolation makes pain worse
Loneliness and chronic pain can cause a vicious cycle: you have to cancel plans due to pain, then become more isolated, which further intensifies pain. There are several ways in which loneliness can worsen pain and its experience:
1. Increased stress = increased pain
Isolation is a stressor, and one that is not to be underestimated. Increased stress levels increase the activity of the body’s stress system (the HPA axis), which can actually increase your sensitivity to pain. This is not just ‘in your head’, but a legitimate increase in your pain levels.
2. The brain processes social and physical pain in a similar way
Research has shown that social pain (like rejection or loneliness) and physical pain share overlapping brain pathways. So, when you feel socially disconnected, your brain may literally process it in a similar way to physical pain.
3. Decreased ability to use social support, even when it’s available
When you feel isolated, your perception of others may become more negative:
- You may come to expect rejection and stop trying to connect as a result
- You may withdraw entirely and reject others yourself
- You may struggle to accept help
This creates a cycle where support becomes less accessible, even if in theory it’s there.
Chronic pain can feel even more isolating if you’re:
- An expat or immigrant
- Living far away from ‘your people’
- Already feeling a bit out of place or navigating identity questions about queerness or neurodivergence
In these cases, it might be even more difficult to feel understood or explain your experience to others.
The good news: why social support helps
The flip side of the coin is that social support can act as a buffer, improving your overall quality of life. Social support includes, bit is not limited to:
- Emotional support: listening, understanding
- Practical support: help with daily tasks
- A sense of belonging: being embedded in a community
And research shows that chronic pain patients who perceive more social support report less intense pain, cope better psychologically, and are less stressed.
Support groups: do they actually help?
Research suggests that they do. However, there are also potential drawbacks, so you will need to evaluate for yourself if a support group might be right for you, and do some digging into what is available near you or online. As a rule of thumb, support groups that include both professional guidance and peer-led sessions tend to be the most effective.
Benefits:
- Validation and understanding: you get to talk to people who share a similar experience
- Decreased social isolation
- Improved coping skills: sharing of both practical and psychological tips to help you cope better
- Improved functioning in daily life (including decreased reliance on healthcare professionals)
Potential drawbacks:
- Focus on negative outcomes: shared validation may turn into dwelling on symptoms and hopelessness
- Accessibility issues: especially when it comes to in-person meetings, pain may serve as a barrier to access
- Potential for misinformation and varied group quality: groups that are not led by a professional may spread misinformation. Different groups also vary widely in quality.
Practical ways to support yourself
Chronic pain is very difficult to deal with, and social support will not fix all your problems. However, if possible, making small steps toward a more satisfying social life can help you get a bit more joy out of your life.
1. Focus on quality, not quantity
Rather than trying to hold together a large social network, try to focus on meaningful connections. Ask yourself: “Who is there for me no matter what?” “Where do I feel understood, if only slightly”. Pour your limited energy into people who truly matter.
2. Reduce isolation gradually
Don’t try to overhaul your social life completely, as it can lead to exhaustion and burnout, which can further lead to complete withdrawal later on. Instead, try meeting someone for a quick coffee or message a friend instead of meeting up. Try to let people in, even if just a little. Others can’t understand if you don’t open up.
3. Notice patterns around your withdrawal
Do you tend to isolate when you’re in pain, or is there something else going on as well? Maybe it happens when life gets busy, or after experiences of rejection, perceived or otherwise. Try to keep track of it, and make a plan for what to do is you notice yourself isolating again.
4. Consider more structured support
If you find it difficult to connect with the people around you, or are simply looking for more understanding, consider joining a support group, starting therapy (ideally with a therapist with experience with clients who suffer from chronic pain), or seeking connection on community spaces. The structure might provide some routine into your life, and is an intentional way to increase your sense of belonging.
One thing is clear – chronic pain is complex, it does not have a single cause, just like there is no single solution. The journey can certainly feel hopeless at times, especially if you’ve been struggling for a long time. However, we know that feeling alone can make things worse, and if there are ways you can improve your social connection, even slightly, you might improve how you’re feeling, even if it’s not a big miracle cure.
References
De Heer, E. W., et al. (2018). The association of depression and anxiety with pain: A study from NESDA.
DeVries, A. C., et al. (2003). Social modulation of stress responses.
Dresler, T., et al. (2019). Understanding the nature of psychiatric comorbidity in migraine: A systematic review.
Eisenberger, N. I., & Lieberman, M. D. (2004). Why rejection hurts: A common neural alarm system for physical and social pain.
Finan, P. H., et al. (2010). Daily affect relations in fibromyalgia patients reveal positive affect buffering effects.
Hogan, B. E., et al. (2002). Social support interventions: Do they work?
Lopez-Martinez, A. E., et al. (2008). Perceived social support and coping in chronic pain.
Rzeszutek, M., et al. (2016). Social support and coping strategies in chronic pain patients.
Subramaniam, K., et al. (1999). Peer support groups in chronic pain management.